

|
||||||||||||||||||||
 |
FIGURE 4 - When removing PVNS tissue from the knee joint arthroscopically, a small, motorized tissue resection instrument is introduced into the knee through a 1/4 inch skin incision, or "portal." The surgical work is observed by way of an arthroscope (shown here in the upper right-hand section of the FIGURE), inserted through another skin portal incision from a different angle. Each pair of portal incisions (arthroscope and resector instrument) allows a certain region of the knee joint to be cleaned out, with a comprehensive synovectomy requiring upwards of six to eight access portals |
For patients interested in the technical aspects of arthroscopic knee synovectomy, reprints of my illustrated surgical technique paper, published in Master Techniques in Orthopedic Surgery,can be obtained by either writing or e-mailing our Knee and Shoulder Centers office. Simply stated, the objective of arthroscopic synovectomy is to remove as much abnormal joint lining tissue as is technically feasible without damaging the patient's knee in the process. Properly and meticulously performed, it is a very lengthy and technically difficult surgical procedure. It requires mastery of almost every knee access technique ever devised by arthroscopic surgeons. All of the major internal regions of the knee joint, in sequence, must be both visualized and accessed by surgical re-section instrumentation, all the while keeping the number of access (arthroscope portal) incisions to a minimum and avoiding unintended neurovascular injury or damage to other internal joint structures. The surgeon must be comfortable working in the posteromedial and posterolateral knee compartments (see FIGURE 5) and have the patience to follow the abnormal joint lining tissue down into every accessible fold and recess elsewhere within the knee joint. When PVNS disease afflicts the cruciate ligaments, the synovial lining membrane of these ligaments must be carefully and meticulously dissected away (both in the front and sometimes in back) without damaging the ligaments themselves (see FIGURE 6).
 |
FIGURE 5 - This illustration shows another step during the course of a comprehensive, internal knee synovectomy. Here, the arthroscope (left) is being inserted into the posterolateral (rear, outside) compartment of the knee directly, while the resector instrument reaches the inner regions of that compartment indirectly by passing through the inter-condylar notch (center space of the knee) from the front. When creating surgical access portals toward the back side of the knee, great care must be taken not to injure the nearby nerves and blood vessels leading to the lower leg. In this picture, the critically important peroneal nerve is seen just beneath the posterolateral arthroscope access portal. Remember that the surgeon cannot actually see this nerve at the time the adjacent skin portal incision is made! He or she must be guided by way of external landmarks and a sound knowledge of internal knee anatomy. |
|
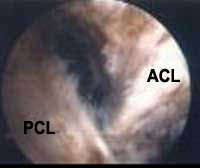
FIGURE
6 - This arthroscopic view demonstrates a patient’s
anterior cruciate ligament (ACL) and posterior cruciate
ligament (PCL), looking from behind, as the arthroscope
has been inserted by way of a posterior-medial portal access
site. These cruciate ligaments were previously surrounded
by PVNS tissue, which was carefully stripped away, both
in front and in back, by way of arthroscopic instrumentation.
|
 |
Clinical experience has generally demonstrated that the more complete the degree of synovectomy achieved, the lower the recurrence rate of the disease. However, even with a consummately skilled surgeon using the most advanced arthroscopic techniques, it is still impossible to remove every last bit of PVNS tissue in the diffuse form of the disease. Current surgery is, therefore, limited to a thorough "debulking"process that falls short of total resection. The surgeon attempts to achieve the greatest possible debulking effect in order to minimize the recurrence rate,while still leaving the patient with a functional knee afterwards. Why the disease does not recur in all cases, following what we know to be less than a 100% synovectomy, is unknown. Diffuse PVNS is truly a strange disease that appears for uncertain reasons and may also completely exit a patient's life following treatment, even though by definition that treatment is known to have been incomplete. If there has been any common etiologic (causal) thread in many of the PVNS patients I have treated, it has been that they had some episode of knee trauma in their past that caused bleeding within their knee joint. Whether a brief exposure of a synovial joint to the iron-based hemoglobin pigment released by degrading red blood cells can actually cause PVNS has never been proven and at this point must be relegated to personal speculation.
Other means of treating pigmented villonodular synovitis include radiation beam therapy and radio isotope synovectomy. In the latter procedure a liquid, radioactive isotope is injected into the knee joint, subjecting the synovial lining to radiation treatment. This is an uncommon treatment that in the past has generally been reserved for difficult cases of PVNS that have recurred following a prior surgical synovectomy. Very few medical centers in the United States even offer such treatment, which is usually done under carefully controlled conditions in research protocols. Either form of radiation therapy can also be used as an adjuvant (additional or back-up) treatment following a surgical synovectomy.
If PVNS remains uncontrolled, over a period of years the patient's knee joint surfaces may gradually become destroyed, leading to a need for radical joint resection and replacement by prosthetic components ("total knee replacement" surgery). The initial radical resection stage of such a procedure allows relatively complete exposure inside the joint and thus an unusually complete surgical synovectomy. This often leads to a final cure of the disease, but the original knee joint has been lost forever.
In this author’s experience, a recurrence of diffuse PVNS
following an initial synovectomy procedure is still worth treating
with another attempt at a comprehensive arthroscopic synovectomy,carried
to the most radical extent that is feasible. In some cases unusual
measures such as resecting the soft tissue from behind the posterior
cruciate ligament must be performed, as that is a site where nests
of PVNS tissue may form and even begin to reach outside the
confines of the knee capsule. Resection of such extra capsular
(outside of the knee joint proper) PVNS tissue with an arthroscope
is an extremely tricky process, particularly in the posterior
regions of the knee joint where the major neuro vascular structures
that feed the lower leg and foot are located. Most scientific
articles and book chapters on PVNS do not even discuss the fact
that PVNS tissue can occasionally escape the confines of the joint
cavity to invade soft tissues outside of the capsule. While it
is well known that PVNS tissue can actually grow into the femur
or tibia itself, apparently by following vascular (blood vessel)
channels into the bone, it is less commonly appreciated that PVNS
tissue can grow along small, trans-capsular passage ways leading
out of the knee joint cavity to form masses of tissue in external
regions. Two such regions are known as the lateral popliteus recess
and the medial gastrocnemius-semimembranosus bursa (see
FIGURE 7). Extra-capsular extensions of PVNS disease are
best detected pre-operatively by way of MRI scanning with special,
hemosiderin-weighted imaging techniques. If identified, such extra-articular
nests of PVNS tissue are usually best resected by way of localized,
open surgical exploration, leaving the intra-articular PVNS tissue
to be resected by arthroscopic means.
 |
FIGURE 7 - This MRI scan shows a cross-sectional, side view of a knee. The rounded femoral condyle sits atop the flat upper tibia. The front of the knee is to the right and the back of the knee is to the left. The arrow points to an accumulation of PVNS tissue outside of the knee joint, filling up a natural pouch or space known as the gastrocnemius-semimembranosus bursa. The PVNS tissue appears black in this MRI study. If you look within the knee joint cavity in front of the femur, you will see additional, dark PVNS tissue, in a more typical location. This patient was treated with a comprehensive arthroscopic synovectomy inside the joint followed by excision of the extra-articular mass of PVNS tissue (arrow) using an open, posteromedial skin incision and exploration. Six years after surgery, this patient was symptom free and an apparent cure. |
Resolution of the disease process is usually heralded by an elimination of the patient's prior recurrent knee effusions (excess joint fluid accumulations). Post-operative MRI scans are extremely difficult to read because of scar tissue artifact. If at some point excess knee joint fluid begins to return, this is suggestive, but not definitive proof of, recurrence. If long-lasting, the presence of recurrent fluid suggests the need for a follow-up MRI scan and an arthroscopic re-inspection of the joint. For recurrent disease, a combination of repeat synovectomy, possibly followed by irradiation or radioisotope, adjuvant synovectomy, can be considered. Individual consultation between the patient and the subspecialists at those few medical centers offering the latter technique is required to determine whether the patient is a potential candidate for this treatment.
|
|
||
|
If you have either confirmed or suspected PVNS, getting expert, orthopedic subspecialty care is always advisable! If you have questions concerning your own or a family member’s knee condition, you are invited to have those questions answered by way of a consultation here at The Knee and Shoulder Centers. We have anatomic charts, models, and educational video tapes available to help you participate actively in the medical assessment and decision-making process. |
||
|
|
||
|
|
||
|
|
|
|
|
|