
|
||||||||||||||||
 |
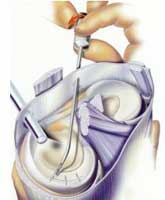
FIGURE 4 - This picture demonstrates the top portion of a tibia, upon which are resting the medial and lateral menisci. A peripheral, longitudinal (parallel to the meniscal curvature) tear in the medial meniscus is shown in the process of being suture-repaired. The femur is not shown here, so as not to obstruct a full view of the menisci. Note that the tear is relatively even and linear, and located in the outer 1/3 (or so-called "red" zone) of the meniscus, which makes it ideal to repair. Tears in the inner, thinner 2/3 of the meniscus (immediately to the left of the tear shown here) would be far less likely to heal if repaired because this portion of the meniscus does not have a capillary blood supply. |
 |
| FIGURE 5 - Diagrammatic illustration of an arthroscopic meniscus repair technique using bioabsorbable (slowly dissolving) meniscus repair darts or "arrows". |
The general internal environment of the knee at the time of repair seems to have some effect on the chance for successful meniscus healing after surgery. It has been found that meniscal repairs done at the same time as surgical reconstruction of the anterior cruciate ligament have a somewhat better chance of long-term success than meniscal repairs done by themselves. This may be due to biochemical healing factors that are more active within a knee joint that has been irritated in a more extreme fashion by way of more extensive injury and surgery.
Aside from good surgical technique, the key to obtaining a high success rate with meniscal repair is often as simple as using selective judgment when making the decision to repair versus remove. All possible effort should be taken to repair otherwise healthy menisci that have excellent healing potential, whereas effort should not be wasted on thoroughly degenerated menisci that have no realistic chance of healing well and/or functioning normally. The decision whether or not to attempt repair in a "borderline" case (i.e., adequate healing is unlikely but not impossible) can involve some input from the patient, as well as consideration of the patient's specific circumstances. The younger the patient, the more consideration should be given toward meniscal repair, as loss of meniscal function sets in motion an accelerated aging process within the joint that leads to at least some degree of future osteoarthritis in the affected region of the knee. In an older individual (over 35 or 40) who is not overweight and who has no leg malalignment ("bowleg" or "knock-knee" deformity) a "borderline" meniscal tear with a sub-par chance for healing after meniscal repair is often best treated by primary meniscectomy. This is because the patient's knee has probably already been subjected to the majority of stresses that it will see during the course of its lifespan, and it has no specific risk factors (other than the meniscus injury) for premature osteoarthritis. This makes the loss of meniscal cushioning less objectionable. One must also consider the greater risk of surgical complications associated with meniscal repair procedures (vs. simpler and quicker removal procedures) and the extra surgical risks that the patient would be subjected to if a second procedure were to be required because the repair of a "borderline" tear ultimately failed. Even under ideal circumstances, a surgically "repaired" meniscus is not guaranteed to heal!
When deciding whether to repair or remove problematic meniscus tissue, each patient's case must be considered individually, taking into account the patient's circumstances and wishes, the degree of pre-existing meniscal degeneration evident, and the overall physical condition of the knee at the time it is first inspected arthroscopically. Your surgeon's knowledge and expertise are also important!
|
|
||
|
If you have been diagnosed with a knee meniscus "tear" and you would like a second opinion concerning it’s potential for preservation or repair, do not hesitate to call upon us here at The Knee and Shoulder Centers. |
||
|
|
||
|
|
||
|
|
|
|
|
|