
|
|
a. |
performing a manual ligament stress examination while
the patient is under anesthesia, carefully comparing
the injured knee to its normal mate, and; |
|
b. |
while viewing the ACL with the arthroscope, palpating and probing it with a blunt instrument as it is tightened (stretched) by external knee stress - if it becomes taut and rigid rather than remaining lax and soft, it has retained some significant portion of its mechanical integrity. |
Thermal (heat-induced) ligament shrinkage/tightening procedures
for loose or stretched out cruciate ligaments have not yet been
proven effective over the long term and have occasionally been
reported to cause ligament necrosis (tissue death) followed by
complete dissolution or rupture. They should, therefore, be approached
with caution.
Related Ligament Injuries and Complex Instabilities
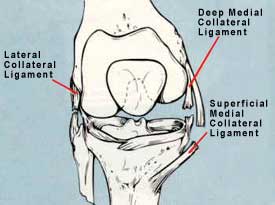 |
| FIGURE 10 -Diagrammatic illustration of how one or more collateral ligaments can be torn in combination with a cruciate ligament injury. |
In particularly severe knee sprains, there is usually more damage
than just a ruptured anterior cruciate ligament. In some cases
additional ligaments such as the medial collateral (inner-side)
ligament, posterior cruciate ligament, lateral collateral (outer-side)
ligament, or portions of the joint's capsular (surrounding envelope)
ligament are traumatically compromised as well (see
FIGURE 10). The decision whether or not to perform surgical
work on these additional damaged structures at the time of ACL
reconstruction requires a good deal of insight and experience
on the part of the surgeon, as this decision is often a "judgment
call". Surgery to correct collateral ligament and capsular
defects or laxities is known as "extra-articular" (external
to the joint cavity) repair and/or augmentation, and is done in
addition to the "intra-articular" anterior cruciate
ligament reconstruction within the joint cavity. While formerly
performed with great frequency (and often to the exclusion of
intra-articular ACL reconstruction), supplemental extra-articular
surgery today is not commonly performed. To some extent it has
become a "lost surgical art." Few orthopedic textbooks
describe methods of rebuilding a chronically torn medial collateral
ligament, and very few surgeons have much experience in performing
this type of surgical work. Various supplemental, extra-articular
reconstructions involving "reefing" (capsule
over-folding and tightening) and "tenodesis"
(converting a nearby tendon into an auxiliary ligament) procedures
may be needed when attempting to treat a knee that demonstrates
a more severe (complex or multi-directional) instability as compared
to a simple, isolated anterior cruciate ligament laxity. The older
(more chronic) the ACL tear is, the more likely "complex"
instability will be encountered. The experienced reconstructive
knee surgeon will know when such supplemental procedures are likely
to contribute to a successful outcome and which particular method
to perform.
|
|
|
|
|
|