
|
||||||||||||||||||||||||||||
 |
FIGURE 5 - As viewed with the arthroscope (femoral condyle above and tibial articular surface below), OCD lesions that have not overtly loosened or separated may actually be difficult to locate. The arrows here point to a slight bulge in the normal curvature of the femoral condylar surface, which in this patient was the only visible sign of a very large, underlying OCD lesion that was quite obvious on an MRI study. This patient went on to have a retrograde bone grafting and screw fixation procedure (see Figures 6 and 7), which resulted in complete healing of the lesion before it ever had the chance to grossly loosen or separate. |
One way of treating stable and relatively stable lesions is by a drilling a number of small holes through the involved articular surface, proceeding down through the OCD ossicle and fibrous tissue interface into the normal bone of the parent femur. This is done in the hope of creating internal bone bleeding and an inflammatory healing reaction that ultimately fixes the underlying bone ossicle into its crater (the two bone surfaces will hopefully "knit" together, as would a fracture). This approach has the disadvantage of potentially compromising the otherwise healthy, articular cartilage cap over the OCD ossicle by way of the multiple, drill-hole punctures. Another, more technically difficult approach is to perform "retrograde" (coming in from behind) "bone grafting" of the lesion. Bone grafting refers to a process where healthy bone tissue is transplanted from an area where it is expendable, to an area where bone is deficient and/or unhealed. The OCD lesion is approached by drilling a small tunnel through the femur, starting at a distant location and approaching the lesion from behind. The drilling must stop just as the tunnel passes through the lesion's fibrous interface layer, reaching the necrotic (dead) OCD nucleus, or else the drill may go through the ossicle and exit out through the articular surface cartilage, thus damaging it. This procedure requires fluoroscopic (x-ray) guidance during drilling (see FIGURE 6) and direct visual confirmation that the fibrous interface has been reached and breached by the drill bit. This is accomplished by inserting the arthroscope directly down into the bone tunnel to inspect its depths.
 |
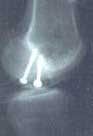
FIGURE 6 - This fluoroscopic x-ray taken during surgery demonstrates a side-view of the same patient's knee as shown in Figure 5. Having located the OCD lesion within the femoral condyle, special reference point markers and x-ray guidance were used to drill a tunnel into the back side of the OCD lesion from a remote location well away from the joint surface. The x-ray demonstrates the furthest extent that the drill was inserted. Once the drill was removed, a direct view down the bone tunnel with the arthroscope confirmed that the tunnel had crossed the fibrous interface layer and entered the ossific nucleus of the OCD lesion. The bone tunnel was then packed with bone graft to stimulate healing of the OCD lesion back to the parent femoral condyle. |
A small amount of local femoral bone graft is then harvested
from an area near the tunnel entrance and pushed down to the bottom
of the tunnel. It is packed into the area where the fibrous tissue
interface layer previously existed. This creates a bone tissue
bridge between the ossific nucleus of the lesion and the parent
femur, hopefully allowing rigid, local bone-to-bone healing that
will spread and ultimately result in reunification of the entire
ossific nucleus to the parent femur without ever having disturbed
the overlying articular cartilage cap.
|
FIGURE
7 - X-ray of the same femoral condyle shown in Figure
5, after arthroscopic placement of fixation screws into
the OCD lesion had been performed. The screws were removed
ten weeks later and the OCD lesion was found to be firmly
healed and stable.
|
 |
For large lesions that are not completely stable but have not yet developed overt perimeter fissuring of their articular surface cartilage, the retrograde bone grafting technique can be supplemented by internal fixation and stabilization of the fragment in situ (right where it lies) by way of either removable, stainless steel compression screws (see Figure 7) or bioabsorbable (slowly dissolving) pins or compression screws. This requires that one or two, very small holes be drilled through the articular cartilage cap of the lesion for screw placement, but this is still probably less traumatic to the joint than drilling many holes through the cartilage cap, as is performed in a typical anterograde (frontal approach) drilling procedure. The screws hold the fragment rigidly in place to foster osseous union (healing or "knitting") at the bone graft site. Non-absorbable screws are typically removed after eight to ten weeks by way of the arthroscope, and at that point the lesion can be probed and checked for stability. If micromotion of the fragment is no longer present, then early healing can be assumed to be taking place and the patient can very gradually be allowed to resume weight-bearing activities. During the time the screws are in place (assuming proper screw position and grip), the patient can swim and bicycle without harm to their knee, but they should not bear weight on that leg. With absorbable screws a follow-up arthroscopy may not be necessary, but this eliminates the chance for the surgeon to check the early stability and healing of the lesion directly. Because it takes a long time (six to twelve months) for healing to be clearly recognizable by way of x-ray or an MRI scan, not having the opportunity to recheck the patient's knee arthroscopically leaves the surgeon with less information to go on when instructing the patient with respect to their return to weight-bearing activities.
In cases where the OCD lesion is clearly unstable and the overlying articular cartilage cap has begun to separate by way of circumferential perimeter fissuring, a somewhat simpler (but still difficult to perform) bone grafting technique can be employed wherein the bone graft tissue is introduced arthroscopically into the OCD defect from the front, as opposed to an indirect approach from behind the lesion. Such lesions are often found incompletely separated, hanging on by one area of articular cartilage or fibrous tissue near the intercondylar notch (the central, open concavity in the end of the femur). This acts like a hinge, allowing the lesion to be flipped open as would a trapdoor, thus exposing the base of the crater in the parent femur and the undersurface of the un-united bone ossicle or cartilage cap (see FIGURE 8).
|
|
FIGURE 8 - Arthroscopic photo of a different patient whose femoral OCD lesion had already experienced perimeter fissuring and had become grossly loose. The underlying bone ossicle had completely re-absorbed, leaving only a thick cartilage "cap". The cartilage cap here is opening up on an unseen hinge of partially intact surface cartilage, much like a "trap door". |

The surgeon will carefully hold the lesion open,scrape out any fibrous tissue present (see FIGURE 9) and then insert fresh local bone graft material into the crater (see FIGURE 10). This bone graft material must be very carefully inserted so as to fill up (but not overfill) the empty space created by the removal of the fibrous tissue. The OCD cap must then be closed back down and held in place with internal fixation screws or pins before any of the bone graft material escapes (see FIGURE 11). The greater the degree of prior reabsorption of the dead ossific nucleus, the more fibrous tissue there is to remove and the greater the amount of bone graft material required to fill the void. One must be very careful not to overfill the crater with bone graft or the cap will not fully close back down, causing it to bulge out beyond the normal joint surface contour.
 |
FIGURE 9 - With the cartilage cap (left side) held open to expose the crater in the femur beneath it, the crater and cap are scraped and cleaned of all fibrous tissue. Any dead bone at the bottom of the crater is removed and/or drilled to enhance restoration of local blood supply. |
|
|
FIGURE 10 - This arthroscopic photo demonstrates how fresh (red) bone graft material is inserted into a hinged-open OCD lesion using a modified syringe (the clear plastic tube with the "10" on it). This is a close-up view of the same lesion depicted in Figures 8 and 9. The syringe is withdrawn as the bone graft material is injected into the empty space that remains after the previous removal of dead bone and fibrous tissue. The articular cartilage cap is then closed back down over the bone graft tissue, preventing its escape from the crater. This cap was held in place with two fixation screws, as shown in Figure 11. |
|
|
FIGURE 11 - This was the final appearance of the bone-grafted OCD lesion shown in Figure 10, now held firmly in place with two stainless steel screws. When the screws were removed arthroscopically 10 weeks later, the OCD lesion was healed and stable. The patient was able to run and perform heavy weightlifting six months later with no symptoms of any kind. |


In my experience I have come across two unusual OCD lesions (one of which is shown above in FIGURES 8-11) where the entire ossific nucleus had been reabsorbed, leaving only a thick cap of articular cartilage. In both cases, bone grafting and internal fixation still successfully resulted in firm union of the articular cartilage cap to the parent femur and an ultimate clinical success. As of the time of this writing, I have never encountered an OCD lesion that failed to unite when bone grafting methods were employed, with or without internal screw fixation of the lesion, as needed. Once an individual with at least a partially unstable lesion has reached skeletal maturity by way of closure of their growth plates, I believe that non-operative treatment or less involved surgical approaches (such as simple drilling) are less effective than the more complex techniques utilizing arthroscopic bone grafting.
I have also not yet come across a case where bone grafting and screw fixation of a lesion could not be done arthroscopically, as opposed to opening up the knee by way of a large incision known as an arthrotomy. Such arthroscopic procedures can be lengthy and tedious, and somewhat akin to building a model ship in a bottle, but the post-operative morbidity experienced by the patient (pain, swelling, stiffness and scarring) is usually significantly less and the cosmetic results to be obtained are superior to any procedure that involves an arthrotomy (an important factor to many teenage females).
If an OCD lesion comes completely loose, creating a free fragment within the knee joint, the fragment should be carefully checked with an arthroscope to see if it still has the appropriate size and shape to fit back into its crater in the femoral condyle. If so, then bone grafting and internal fixation methods should be employed to try to replace the fragment in its bed and get it to heal. If that is not feasible, then it must be removed from the joint. The base of the empty crater can be abraded somewhat to make it bleed and thereby provide for subsequent in-filling by fibrocartilage (cartilage scar) tissue, but that almost never provides a good weight-bearing surface and ultimately degenerative joint arthritis will ensue. A possible salvage option in this situation is packing bone graft material into such an open crater to a level just slightly below the level of the surrounding surface articular cartilage, hoping that a surface cartilage layer will form over the solidifying bone graft. Another possible salvage option in such a circumstance is to perform an "OATS" (osteo-articular transplant surgery) procedure (see FIGURES 12a-12d).
 |
| FIGURES 12a-12d - An arthroscopic photo-series demonstrating how an articular surface defect can be treated by Osteo-Articular Transplantation Surgery (OATS). Here, a damaged zone of femoral surface cartilage and a plug of bone beneath it are removed and replaced by an identical sized plug of healthy surface cartilage and underlying bone, harvested from an undamaged donor (non-critical) area elsewhere in the same knee. The final photo demonstrates the round, transplanted plug snugly in place, a perfect fit. If the transplant "takes", the treated area of joint surface has effectively been renewed. |
During such surgery one or more plugs of healthy articular cartilage and underlying subchondral bone are transplanted from less important articular surface areas in the knee (donor zones) to the open crater left by the osteochondritis dissecans lesion, which usually occupies a more critical, weight-bearing zone of the joint surface. Some surgeons are also using one or more small OATS plug transfers as a substitute for the multiple drill-hole or retrograde bone graft procedures mentioned earlier for the treatment of stable, in situ OCD lesions.
It is worth remembering that the goal of each and every treatment for osteochondritis dissecans is to preserve or restore a normally contoured, well supported, weight-bearing articular cartilage layer so that the gliding/load-bearing function of the joint surface is not compromised. It is currently believed that success in this regard will minimize the long-term development of degenerative arthritis.
|
|
||
|
If you have been diagnosed with OCD and / or have undergone unsuccessful treatment for this condition, experienced help is available here at The Knee and Shoulder Centers. |
||
|
|
||
|
|
||
|
|
|
|
|
|